By Anna Gallinat.
We all know health inequalities exist and persist. Systematic differences in people’s health occur between socio-economic classes or geographical areas, although there are other inequalities, for example concerning gender and ethnicity. It has been argued that reducing the health gap means to protect and promote the health of the poorest. The recent 7th European Alcohol Policy Conference (EAPC) addressed the relationship specifically between alcohol and health inequalities. Both issues play a major role in sustainable development, the functioning of our societies and the sustainability of our health systems.
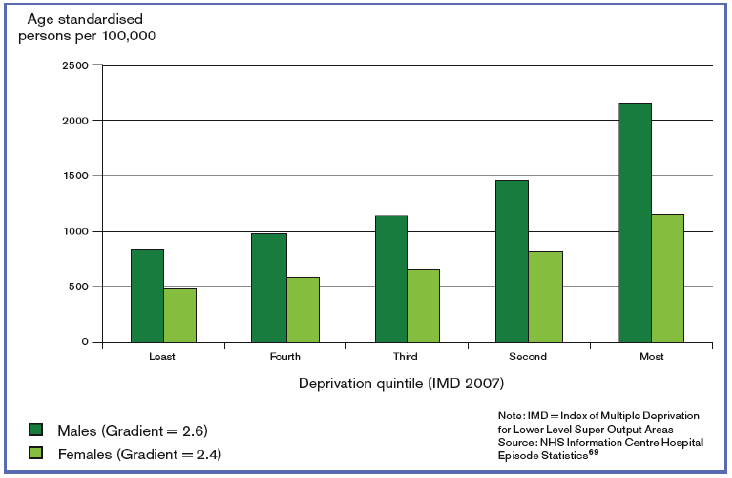
Research has shown that people living under the poverty line often engage in unhealthy behaviours. While this is true for poor diet, smoking, and lower levels of physical activity (Buck & Frosini, 2012), the picture is reversed for alcohol consumption. The highest portion of alcohol consumption is not among the most deprived groups, but rather in the middle and high income groups (IAS). However, according to the Marmot Review (Fair Society, Healthy Lives), alcohol attributable hospital admissions are in fact higher with increasing levels of deprivation (see Figure 1). The same relationship can be drawn up for mortality, disease burden, and harm to others. This means that most deprived groups experiencing higher rates of alcohol harm, while well-off communities consume more but suffer less from the adverse effects of alcohol.

In Figure 2, the proportion of increasing and higher risk drinkers declines as levels of deprivation increase, yet alcohol related mortality moves in the opposite direction and grows with deprivation (IAS). Katherine Brown, Director of the Institute of Alcohol Studies and author of aforementioned report, asked: “This creates something of a paradox; why should some groups experience worse alcohol related harms, despite apparently consuming less alcohol?”
Several theories explaining this so-called alcohol harm paradox exist.
- Materialist: Those with fewer resources (be it social, economic or environmental) are less protected to cope with adverse effects of alcohol.
- Inaccurate consumption reporting: Self-reports and omission of some high prevalence groups, e.g. people experiencing homelessness. Studies are often criticised for not being accurate in this area.
- Other unhealthy behaviours: When adding alcohol into the mix of other harmful behaviours, alcohol acts as a catalyst, accelerating and multiplying negative effects rather than just accumulating.
A fourth theory, relating to a stereotypical view of drinking patterns, that is of binge drinking in lower Socio-Economic Status (SES) groups and more regular drinking among higher SES groups, has not been substantiated by research.
Europe remains the leading region in alcohol consumption with an average 10.9L of pure alcohol consumed per capita and year compared to the 6.2L global average (WHO). At the 7th EAPC, Chris Brown from WHO Europe showed data that 1.3% of GDPs is spent on alcohol related harm in the EU. That is 125 billion Euro per year, which counties (have to) devote to an avoidable and preventable cause. Human lives continue to be lost as well: one in every 17 deaths are because of alcohol harm, accounting for 5.9% of global deaths.
One reason for this is that “Alcohol has never been more affordable and available than today!”, according to Jürgen Rehm, Director of the Institute for Mental Health Policy Research and Professor at University of Toronto.
The problem is not that we, as societies, are unaware of the problems or don’t know how to address them. We know what the three ‘best buys’ for measures which prevent alcohol related harm thanks to recommendations by WHO: regulate availability, marketing, and pricing. At the 7th EAPC, campaigners and policymakers alike presented examples of the implementation of these three best buys across Europe. The case of Minimum Unit Pricing (MUP) in Scotland was often mentioned – both to address alcohol related harm as well as health inequalities.
Raising the price of alcohol, e.g. by the introduction of a special tax or MUP, is an effective policy measure countries can take to tackle these issues and the Scottish Government is one of those following the WHO’s best buy recommendation. In this case, political will and leadership proved to be as vital as coordinated and effective partnership with NGOs, according to Eric Calin of the Scottish Health Action on Alcohol Problems. His colleague Peter Rice refuted the argument that MUP is an “attack on the poor” by making (cheap) alcohol less available. Data shows that cheap alcohol is mainly bought by heavy drinkers, who can be found across all income groups, not just the poor. For Martin Seychell, Deputy Director General at the European Commission (DG Sante), MUP is a social measure as much as a health measure, showing once again the need and success of an intersectoral approach to tackle both health inequalities and alcohol related harm.
As the always inspirational Sir Michael Marmot put it in a nutshell: “If we want to do something about the social distribution of alcohol related harm, we have to do something about health inequalities!”
Further links
Report of the Institute of Alcohol Studies: http://www.ias.org.uk/uploads/pdf/IAS%20reports/IAS%20report%20Alcohol%20and%20health%20inequalities%20FULL.pdf
Podcast of Sir Michael Marmot: https://soundcloud.com/instalcstud/alcoholalert-112014

Anna Gallinat
Anna Gallinat is Communication Project Officer in the Information and Communication unit at Eurofound since February 2018. She supports and works across the various teams in the unit to ensure a coordinated and strategic approach in Eurofound’s outreach activities. She also drafts communication outputs on various cross-cutting topics, such as gender, COVID-19 or EU policy.
Previously, Anna worked at EuroHealthNet in Brussels, where she was responsible for communication and project management for EU health-related projects. She has a Bachelor’s Degree in Psychology from the University of Twente in the Netherlands. She is also a graduate in Gender and Media Studies from the London School of Economics and Political Sciences.