
Improving public health requires a shift from focusing on individual behaviours to creating environments that support healthier choices. It is not just about encouraging individuals to quit smoking, maintain physical activity levels, or vaccinate their children; it is about shaping the environments in which these health-related behaviours take place. By making healthy food more accessible and affordable, integrating healthy eating into education, and providing clear information about school services and food policy, we can create a supportive environment that nudges individuals towards healthier choices.
Improving public health requires a collective effort to create healthier environments. This shift in mindset is crucial for fostering sustainable change. Senior Staff Member, Lien Van der Biest, from the Flemish Institute of Healthy Living in Belgium provides valuable insights into how Flanders is implementing innovative approaches to improve healthy living.
From quitting smoking to maintaining physical activity levels to feeling uncertain about vaccinations, we all know that improving public health comes with behavioural changes. But it's not just about individuals changing their health behaviours, it's also about creating environments that support behavioural changes and healthier choices. After all, the environment we live in forms the context within which these health-related behaviours are to take place, and can either support of undermine them. Do children have the opportunity to eat warm meals at school and how affordable is this service? Are there enough alternatives for lunch such as veggie, vegan or halal options?
If we want to support lasting changes, we need to address these root causes and adapt the environment. We need to make healthy food more accessible and affordable, support teachers in integrating healthy eating in the lessons and inform parents and children about school services and food policy. Importantly, adaptations in the environment also require behavioural changes. Not from the general population or certain risk groups, but from environmental agents that hold the power of shaping the environments in which we live and in turn impact our health choices.
Tackling the complexities of health equity
Being trained as a health psychologist, my strength lies in understanding people and their individual behaviours with regards to their (health-related) life goals. Working within the field of health promotion, one of the things that has struck me is how strongly intertwined both individual health determinants and environmental health determinants are. Let's take obesity prevention for example. Maintaining healthy diets and physical activity depends on complex interactions between individual and environmental determinants. Health literacy, healthy food environments (at home, school, work, or in the public area), food pricing, incentives for active transportation, cultural norms, habits, walkable neighbourhoods - all of these factors play a role in healthy living.
On top of that, most of these health determinants are not evenly distributed, and this leads to massive health inequities. For example, people in socially vulnerable situations may have limited health literacy, live in neighbourhoods with limited healthy food options and increased advertising for unhealthy foods, and experience heightened road unsafety compared to the general population. In addition, they might not be able to prioritise healthy cooking and exercising, due to stressors (e.g. financial) that limit the mental bandwidth that people need to make advised long-term health choices. Along with this, health providers including preventive healthcare services may not be sufficiently accessible to them.
A behavioural and cultural lens to health challenges
The power of our environments to determine, undermine, or support health-related behaviours is undeniable. If we want to tackle the health challenges that threaten us today (e.g. diabetes, coronary disease, obesity, cancer, etc), the onus should not be put on individuals to live healthier. We need to prioritise the creation of health-supportive and equity-supportive environments. Environments in which living healthy is easy, normal and attractive.
Throughout the past years, I’ve become convinced that, by integrating multidisciplinary views on health promotion and disease prevention such as sociology, psychology, anthropology etc., we can better understand the complex interactions between health determinants. It is my belief that behavioural and cultural insights (BCIs), coming from those perspectives, can provide a useful lens to better understand the unequally divided individual and environmental barriers to a healthy life. Systematically incorporating a BCI approach can help form strategies that aim to overcome these barriers, while considering the complex relationships between them.
Unveiling behavioral insights with the 'Wheel of Behaviour'
At the Flanders Institute for Healthy Living (Gezond Leven), we support individuals, groups, and communities to overcome health challenges and health inequalities. We do this by providing evidence-based health information, ready-to-use health promotion tools and interventions, as well as policy advice and data collection. Through our ‘Healthy Living Academy’, we also strengthen and bridge the gap between all stakeholders involved in health promotion and disease prevention. Our work is tailored to the context and needs of diverse settings, from healthcare and wellbeing organisations to schools, childcare, workplaces, and municipalities covering a wide range of health topics including behaviour insights and health inequity.
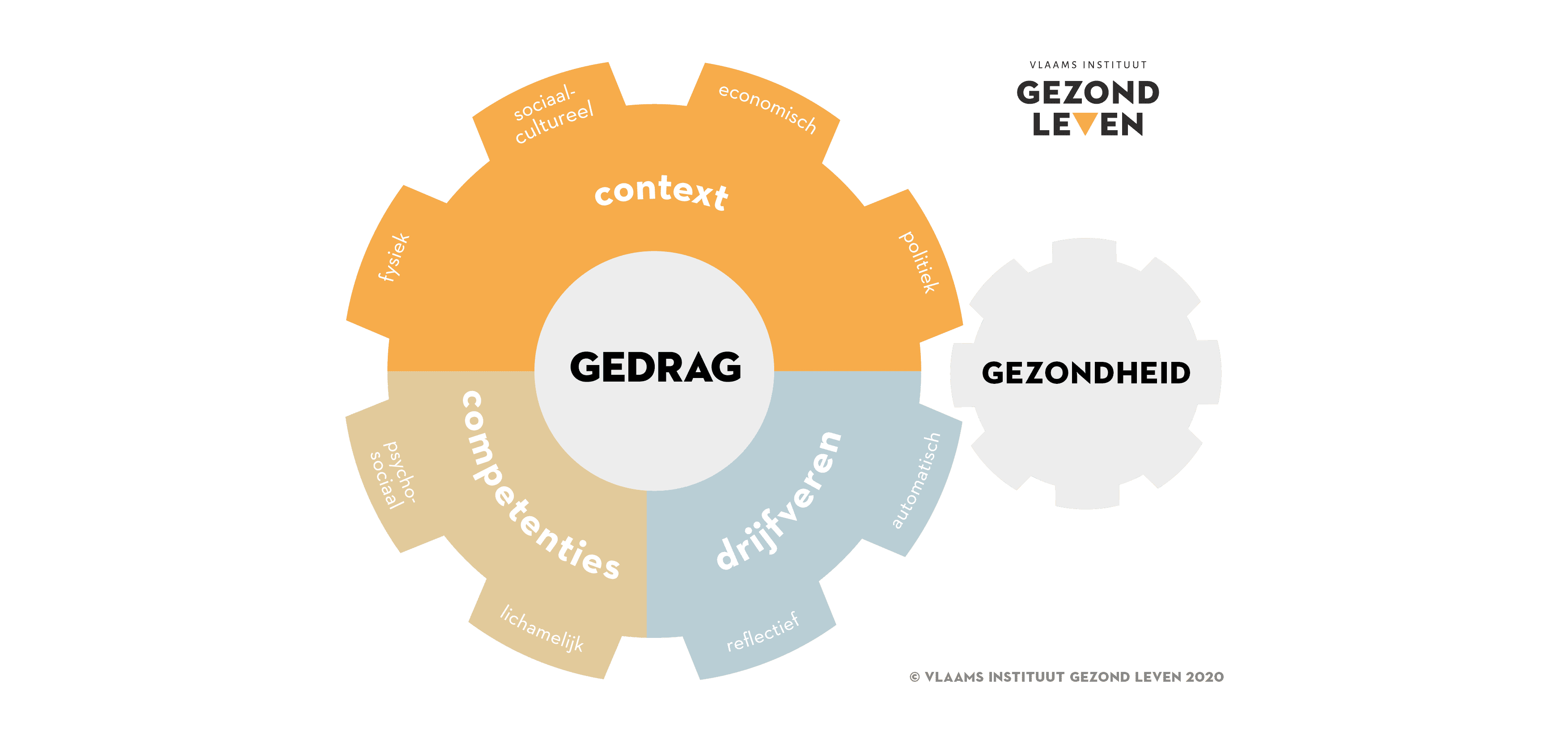
In 2016, the Flanders Institute for Healthy Living set out to make BCI a powerful tool for improving health and wellbeing. First, we needed to build awareness, interest, and support in BCI amongst key stakeholders (members of health promotion and disease prevention organisations, policymakers, researchers, care-providers, …). For me, the best way of doing this was to create a common language, a common image for behaviour insights. This led to the development of the Wheel of Behaviour, a simple but comprehensive model that illustrates how different factors influence health behaviours. Based on Susan Michie and colleagues’ (2013) COM-B model, the wheel places a larger emphasis on environmental factors, such as access to healthy food options, safe and walkable neighbourhoods, and supportive social networks. The model provides a very simple, but comprehensive overview of the types of behavioural determinants that can influence health behaviours, namely the capabilities (within the individual), opportunities (in the environment in which the behaviours are to take place) and the resulting motivation.
This model highlights how behaviours are influenced by both individual and environmental factors, and how this can affect the health of people or populations. The behavioural determinants in the model are universal. Therefore, it applies to all kinds of behaviours: from citizens’ health behaviours such as healthy eating, safe sex, through to the role professional behaviours of healthcare providers or other environmental agents play in the health behaviours of certain target groups (e.g. teachers at school or nurses in hospitals). By understanding and eliminating the barriers that people from both groups encounter in achieving health goals, we can work towards better health and more health equity. This model provides a framework for identifying and structuring these barriers, which is a vital first step in planning health promotion interventions.
Implementing BCIs: a step-by-step approach
To make the Wheel of Behaviour accessible and easy to use, we developed a suite of supporting resources, including a short e-brochure, a more extensive e-learning, an inspiration guide, and a motion graphic. We also incorporated the model into related courses and guest lectures, documents (such as project proposals and reports), and promoted it through print and online media.
The model’s adoption has had a snowball effect, as it has become a staple of primary care programmes in most Flemish universities and colleges, some secondary schools, several health promotion studies and significantly in multiple health promotion interventions in the field. It also sparked exciting and interesting collaboration opportunities, such as the Peul-Chain project, which has successfully demonstrated the power and benefits of BCI approach.
The COVID-19 pandemic was a wake-up call for governments and their approaches to our health systems. The pandemic has been a major driving force for policymakers and other stakeholders, who have started to recognise the critical role of BCIs in public health in Belgium and other nations. Our team has been provided with a unique window of opportunity to advance the use of BCIs in Flanders as a result.
So, what have we done? Our BCI capacity-building package is growing steadily, offering a selection of resources and methods to help people understand behaviour, support behaviour change and evaluate behaviour change interventions. We have also integrated cultural insights and strategies to work towards increased health equity. The package includes information, materials and tools, courses and trainings and tailored advice and partnerships.
The advancement of BCI work in Flanders: next steps
As we plan to advance BCI work in Flanders, we are excited to have recently discovered the ‘European regional action framework for behavioural and cultural insights for health, 2022-2027’. This framework provides a roadmap for using BCIs to create healthier and equitable communities. It represents the first ever commitment on implementing BCIs on this scale.
With its 5 strategic commitments and accompanying progress model, this framework has provided invaluable insights into planning our next steps for BCI work in Flanders. It provides not only evidence-based framework, but also hands-on objectives and practical tools and ideas for achieving them.
We also completed the self-assessment survey based on the progress model, which gave us insights into our strengths and weaknesses in our current BCI work in Belgium. We are ambitious to achieve a higher score on the next self-assessment in 2025 and we know that several advancements are needed to achieve this objective.
Accelerating the application of BCIs
To accelerate the application of BCIs, we are building a dedicated BCI network of key stakeholders across Flanders and Wallonia (federal level), the Netherlands, and the wider European region. This will help us to create understanding and maintain support for BCIs among key stakeholders. Creating a dedicated BCI network in Belgium can help us build momentum for BCIs among key stakeholders (#1 strategic commitment in the WHO framework), bridge the divide between research, policy, and practice, and lay a solid foundation for our next self-assessment in 2025.
The recognition of BCIs extends far beyond the borders of Belgium, where they are already making waves in the realm of public health. The World Health Organization (WHO) Europe is actively nurturing a vibrant community of practice, uniting experts and member states from across the region to translate BCI principles into practical strategies. This dynamic platform, focused on harnessing the power of BCIs, serves as a priceless hub for knowledge sharing, experience exchange, and collaborative efforts.
As BCIs continue to gain traction, WHO Europe's dedication to foster a global network of practitioners is paving the way for transformative change. By bringing together diverse perspectives and expertise, WHO Europe is empowering individuals and organisations to apply BCI principles effectively, leading to a healthier and more equitable world.
Unlocking the economic value for public health
To achieve long-term advancements in BCI work, we need to invest in human and financial resources and build a strong team or unit to lead the change and ensure their sustainability (strategic commitment 4 in the WHO framework). This means advocating for financial support from the government to build a BCI team or unit (depending on government funds), which would greatly facilitate the application and implementation of BCIs.
However, sadly, this is not an easy fix and comes with its challenges. One significant challenge is convincing policymakers to allocate sufficient resources to BCI. Preventive healthcare is already seriously underfunded in Belgium and many other nations, so policymakers are hesitant to allocate more resources to this area.
So, what’s the solution? We need to demonstrate the cost-effectiveness and economic value of BCIs. Show governments how BCIs can be an effective and efficient way to plan health-related policies, services, and communication to improve public health. BCIs can help us understand the factors that influence people's chances of a healthy life and develop more effective health promotion strategies. But proving this is challenging, given the complexity of interactions between health determinants, and the difficulty of measuring the long-term impact of health promotion interventions (especially when working on limited budgets).
Empowering health promoters
To improve the outcomes of health-related policies, services, and communication, we need to invest in the implementation of BCIs among health promotors and other relevant stakeholders. Being behavioural scientists, we are taking a behavioural and cultural approach to the implementation of BCIs. We are asking questions such as:
- Who do we want to support in applying BCIs?
- What does ‘implement’ BCIs exactly mean?
- Who’s already doing this and who isn’t?
- What are the barriers and opportunities to gathering and using BCIs?
- How can we as capacity-builders help?
By exploring these questions thoroughly, we are building a strong foundation for targeted capacity-building efforts.
We will focus our efforts on professionals in preventive healthcare and wellbeing, including primary care-providers (general practitioners, nurses, physiotherapists etc.), examining their educational programmes in higher education, health promotors (e.g., intervention developers), local governments and policymakers, and the organisations they operate from. We will attempt to tailor our training to the interests, professional contexts, and needs of each target group so they can develop the skills and knowledge to use BCIs effectively.
We are not just helping people learn about BCIs-we are building a culture of BCI support. We will offer decision-makers in key organisations to assist them embed BCIs into their structure, culture, and procedures. For example, organisations can support their employees by providing them with software, guides, and tools to assess behavioural determinants in a target group or analyse the effects of a behavioural initiative.
We are excited about the future of BCIs, but we know that changing behaviour is slow and complex. It is not an overnight success which is why it is crucial to share inspirational best practices and bring people together to exchange knowledge and ideas.
We, as health professionals, need to be adaptable and constantly assess the barriers and opportunities to BCI adoption. This includes perhaps having to change our own practices and approaches along the way.
Lessons learned: our BCI journey so far
Get to know your stakeholders’ wants and needs, and tailor your capacity-building efforts accordingly. This means conducting needs assessments, talking to participants, and joining relevant networks. Find out what is hindering and motivating them to use BCIs and plan targeted actions to address those needs.
Include your stakeholders in the process and value their unique insights and potential role to further BCI work. This will help you build a network of BCI champions.
Inspire ‘late BCI adopter’ stakeholders by sharing the success of ‘early BCI adopter’ stakeholders, empowering the latter at the same time. Collect and share good practices and testimonials on applying BCIs to make this happen.
Make it 'NEAR'
- Make it Normal. Show how many people are already using BCIs. This will make it seem less unknown and more mainstream.
- Make it Easy. But not too easy. Provide practical tools and make it easy to get started, but don’t make it so easy that it seems trivial. Make it something that people might want to try.
- Make it Attractive. Make BCI use something to be proud of and illustrate how it can help people to achieve their goals.
- Make it Routine. Incorporate BCI use into organisational procedures and workflows. Make it part of the ‘norm’ and expected part of the job.

Lien Van der Biest
Lien Van der Biest currently works at Flemish Institute of Healthy Living and is a senior staff member of behavioural insights. Lien also did research in Health Psychology, Cognitive Psychology and Behavioural Science.